
Therapeutic Focus

Depression diagnosis
Depression is diagnosed when a person experiences depressed mood and/or loss of interest or pleasure in daily activities for at least 2 weeks and has additional specified symptoms such as problems with sleep, eating, energy, concentration, or self-worth.
First-line antidepressants have limited efficacy and self-limiting pharmacology
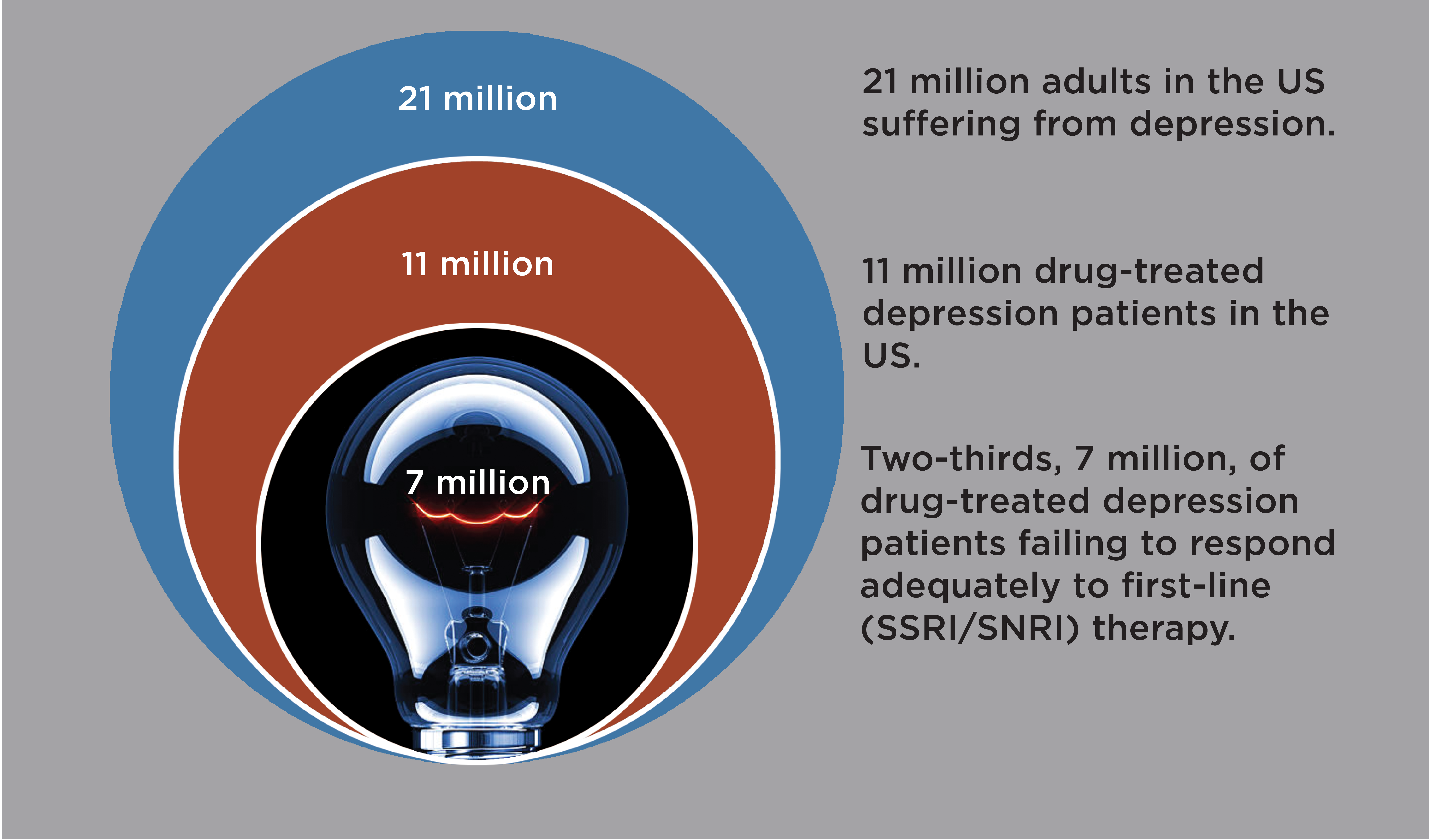
First-line antidepressants (e.g. Prozac®, Paxil®, Cymbalta®) treat depression by blocking serotonin transporters in the brain. Blocking serotonin transporters relieves a brake on serotonin activity. However, serotonin transporter levels are extremely low in the human neocortex(6, 7), only a few percent of levels in the rodent cortex(8). Consequently, in the human brain first-line antidepressants only elevate active serotonin—i.e. extracellular serotonin—modestly, inconsistently, and with a delay(9, 10), and treat depression only modestly, inconsistently, and with delay(11). While some patients respond well, fully two-thirds of patients respond inadequately to first-line antidepressants(11). Increasing dose has no or modest added efficacy, as first-line antidepressants block most serotonin transporters already at standard doses(12). Switching to a different first-line antidepressant or an atypical antidepressant (e.g. Wellbutrin®) enhances efficacy in only a fraction of patients(13). For newer branded antidepressants, e.g., Trintellix® and Auvelity®, there are little evidence for meaningful mechanistic differentiation or therapeutic advantages over generic first-line antidepressants(14-16).
Next-line antidepressants – Limited added efficacy and safety concerns
Atypical antipsychotics (e.g., Abilify®) is the only oral drug class proven and FDA-approved to treat depression responding inadequately to first-line antidepressants(17). Atypical antipsychotics are administrated adjunctively (as add-on) to augment first-line antidepressant therapy. But atypical antipsychotics works well in only 1 in 9 patients(18) and carry safety concerns, e.g., metabolic anomalies and tardive dyskinesias(19).
The urgent need for new outpatient next-line antidepressants
Promising new antidepressant therapies have been FDA-approved, such as brain stimulation and Spravato® (intranasal esketamine), or are in development, notably psychedelics.
Suicidal Ideation
 In 2022, almost 50,000 died by suicide in the US, an all-time high, and more than 1.7 million people attempted suicide(38). Among young people, suicide is the second leading cause of death. Veterans have a 70% increased risk of suicide compared to non-veterans(39). Suicide has risen to epidemic levels and is a national emergency in the US. More than 12.5 million seriously considers suicide in the US every year. Every year 1 million are hospitalized for acute suicidal ideation crisis(38).
In 2022, almost 50,000 died by suicide in the US, an all-time high, and more than 1.7 million people attempted suicide(38). Among young people, suicide is the second leading cause of death. Veterans have a 70% increased risk of suicide compared to non-veterans(39). Suicide has risen to epidemic levels and is a national emergency in the US. More than 12.5 million seriously considers suicide in the US every year. Every year 1 million are hospitalized for acute suicidal ideation crisis(38).
Living under the cloud of suicidal ideation—even if never realized as a suicide attempt or completed suicide—is a life of torment and misery, and represents a critical unmet need in its own right(40).
Unfortunately, there are no FDA-approved drugs for suicidal ideation, suicidal ideation crisis, or to prevent future suicides – albeit IV ketamine may have efficacy(41). As for all Psychiatric drug discovery, the quest for drugs for suicidal ideation are hampered by the lack of animal models. We rely on clinical evidence to inform suicidal ideation drug discovery.
EVX-301 could be the first FDA-approved drug to treat suicidal ideation crisis
Evecxia Therapeutics is developing EVX-301 to treat patients hospitalized for acute suicidal ideation crisis. EVX-301 is designed to amplify brain serotonin with fast onset, which convergent clinical evidence suggest could treat suicidal ideation with fast onset(42-46).